Gastrointestinal Surgery
Procedures
Emergency gastrointestinal
surgery
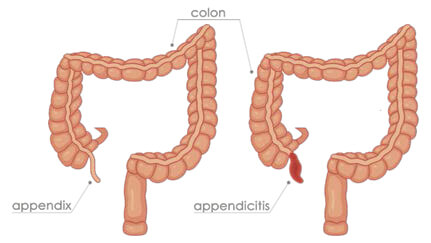
- Acute appendicitis
- Intestinal perforation (duodenal ulcer, colonic perforations)
- Life threatening bleeding of the gastrointestinal tract
- Intestinal obstruction
- Severe infections of the gall bladder
- Trauma to the abdominal organs
Emergency conditions affecting the digestive require emergency surgical intervention. Such
conditions need to be managed by performing emergency laparoscopy or explorative laparotomy
which involves making an open incision to explore the abdominal organs
to treat the emergent problem. Accident and trauma to the abdominal organs may require emergency
surgery to stop bleeding or remove the damaged organ (e.g. emergency removal of the spleen)
Acute appendicitis is one of the commonest acute conditions presenting to the emergency
department. The standard of care is to remove the infected appendix (appendectomy) which is
generally done laparoscopically with excellent outcomes.
Upper gastrointestinal
procedures
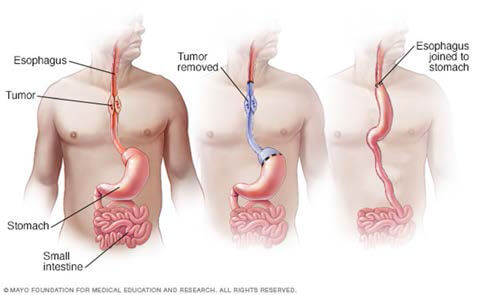
Surgery for Esophageal cancer – Depending on the stage of the cancer, surgical removal of
part of the esophagus offers curative management option. This can be done by laparoscopic or
open surgery either through the abdomen
(Trans-hiatal) or the chest (trans thoracic).
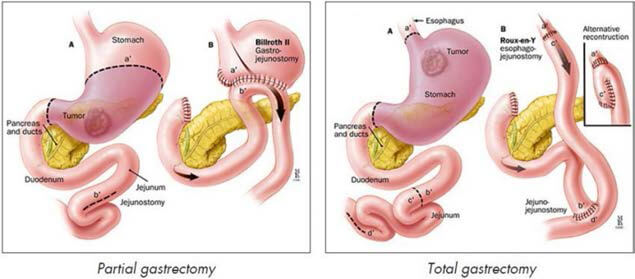
Stomach cancer – Gastrectomy is a procedure where whole (total gastrectomy) or part
(partial / sub-total gastrectomy) of the stomach is surgically removed, generally as a curative
procedure for cancer or sometimes benign
condition. This can be done either as open or laparoscopic technique.
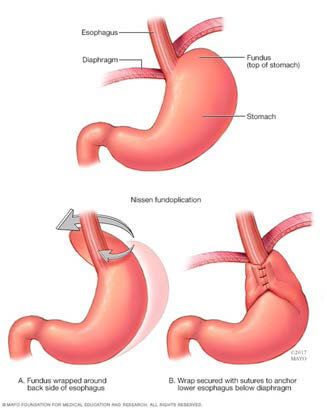
Fundoplication: It is a procedure to treat severe gastro-esophageal reflux disease (GERD)
when maximal medical therapy has failed to improve the symptoms. It is also a procedure
recommended for treatment of hiatus hernia.
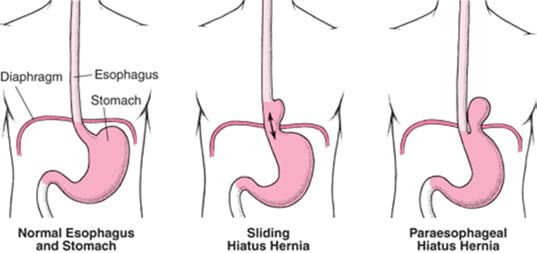
Para-oesophageal hernia repair: Surgery to repair oesophageal hiatal hernia. This type of
hernia occurs due to widening of the gap in the diaphragm through which the oesophagus passes.
This procedure can be performed by laparoscopic surgery.
Surgery for Achalasia Cardia – Heller myotomy is a laparoscopic (minimally invasive)
surgical procedure used to treat achalasia which is a disorder of the esophagus that makes it
hard for foods and liquids to pass into the
stomach due to increased tone of the lower oesophageal muscle sphincter.
Esophageal strictures – Esophageal stricture is a narrowing in the esophagus that can be
caused either by benign or malignant conditions. Depending on the disorder endoscopic therapy is
initially advised and surgical resection
(removal) of the affected area is recommended if endoscopic treatment fails.
Gastrojejunostomy – When there is blockage to the outflow of the stomach and curative
surgery is not an option, then a part of the small intestine is joined to the stomach to by-pass
the blockage.
Small bowel resection – Sometimes, a part of the small intestine may have to be removed
due to either malignant or benign disease; or as part of other procedure (for eg.
Pancreatoduodenectomy).
Feeding jejunostomy – This is procedure where a feeding tube is placed in the small
intestine to facilitate feeding when alternative feeding methods are required either due to
advanced disease or after gastric or esophageal
surgery to help faster recovery.
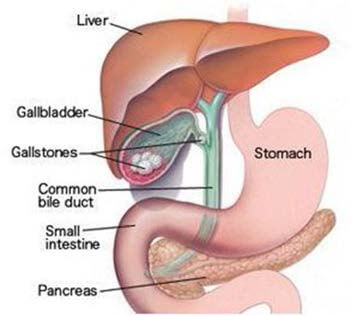
Gall Bladder / Bile ducts
- Laparoscopic Cholecystectomy - Removal of gall bladder for stone disease
- Radical cholecystectomy - Removal of Gallbladder along with a part of the liver and
with lymph nodes for cancer of the Gall bladder.
- Treatment of Biliary injuries – Usually after difficult Laparoscopic
cholecystectomies, injuries to the bile duct can occur. Requires careful management and
reconstructions depending on the type and severity of the injury.
-
Common bile Duct exploration for stone disease.
-
Treatment for cancer of the bile duct - Cholangiocarcinoma
-
Bile duct reconstruction for choledochal cysts which are congenital abnormalities of the
bile ducts with high potential for complications including cancers of the biliary system.
Pancreatic surgeries –
-
Management of Acute Pancreatitis: Severe Inflammation of the pancreas can sometimes
lead to destruction of part of the pancreas which will need surgical removal (necrosectomy).
-
Laparoscopic Cystogastrostomy or Jejunostomy for Pseudocyst of the Pancreas. Usually
performed as a laparoscopic procedure.
-
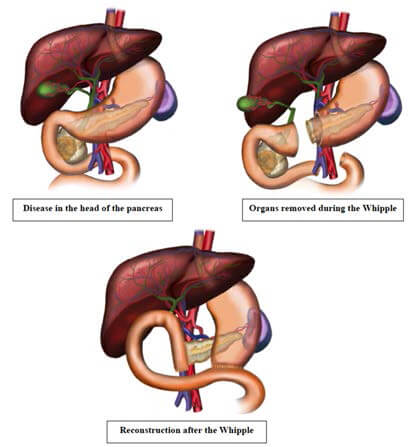
Whipple’s Pancreaticoduodenectomy – Complex surgery for the removal of Pancreatic /
duodenal / distal bile duct cancers.
-
Distal Pancreatectomy – for cancers / tumors of the body and tail of the pancreas.
Spleen can be preserved in most cases. Laparoscopic surgery is standard of care for most
patients.
-
Total Pancreatectomy - involves removal of the whole of the pancreas when it is
completely affected by the disease process.
-
Pancreato-jejunostomy for Chronic calcific pancreatitis – Can provide significant
pain relief and improved quality of life for these patients.
-
Splenectomy – Lap / robotic – for various disorders mostly hematological indications.
Colon and rectal surgeries-
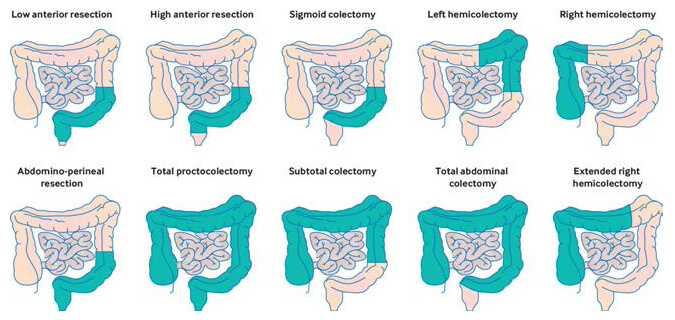
Segmental colonic resections or colectomy: Colectomy is surgical removal of part of the
large intestine or the colon. The indications for doing this procedure would be cancer,
inflammatory bowel disease, diverticulitis,
ischemia (loss of blood supply to the bowel) or life-threatening infections. Depending on the
part of the colon removed, there can be a right or left colectomy or sigmoid colectomy. The ends
of the intestine remaining are joined
together to restore continuity of the tract. In some instances where the ends of the bowel
cannot be joined either due to severe inflammation or infection, then one end of the bowel is
brought out through the abdominal wall as
a stoma. In majority of the cases, this would be a temporary measure and can be reversed at a
later date.
Total proctocolectomy: In severe cases where most of the colon is involved with disease,
a subtotal colectomy or a total proctocolectomy (colon + rectum) is performed. In subtotal
colectomy, the end of the small bowel is
joined to the top of the rectum to restore continuity. In a total proctocolectomy a permanent
stoma (Colostomy) is fashioned or restorative procedure can be performed where in the small
bowel is fashioned in to a pouch (Ileal pouch)
and joined to the anal canal in such a way so as to act like reservoir for the faeces, thereby
avoiding a stoma.
Resection of rectum: The procedure for surgical removal of part of the rectum is called
anterior resection. Depending on the level where the rectum is cut, it can be divided in to a
high or a low anterior resection. When
the tumour is close to the anal passage, an ultra-low anterior resection can be performed which
will preserve the anal sphincter muscles that are essential for faecal continence.
Rectopexy (for rectal prolapse): This a procedure for treating prolapse of the rectum.
Rectal prolapse occurs when the pelvic floor muscles are weak and part of the rectum prolapses
out through the anal passage. There two
ways of surgically treating this. It can be done through the abdomen (Laparoscopically) where
the rectum is supported with insertion of a mesh or through the perineum, where the surgery is
performed through the anal passage.
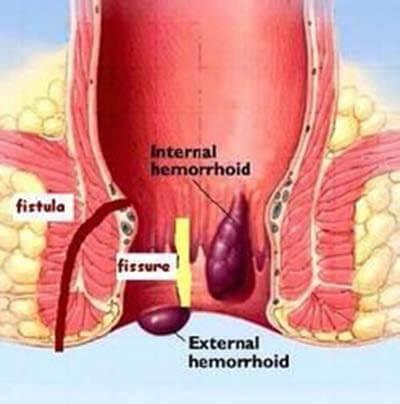
Ano-Proctology: Conditions affecting the anal passage and lower part of the rectum
include Hemorrhoids, anal fistulas and Anal fissure. Haemorrhoid treatment that can be offered
are stapled haemorrhoidectomy (PPH), HALO
(Haemorrhoidal Artery Ligation Operation) and conventional haemorrhoidectomy. For
fistula-in-ano, depending on the involvement of the anal sphincter muscles, choice of procedures
includes fistulotomy (laying open), fistulectomy
(removing the fistula tract), seton insertion (inserting a thread through the fistula tract),
LFT (Ligation of Intersphincteric Fistula Tract) etc. Anal fissure is a very painful condition
and surgical treatment is advised when
medical therapy fails to cure it. Fissurectomy (removal of the fissure) or lateral
sphinchterotomy (dividing part of the internal anal sphincter) can be performed to help cure it.